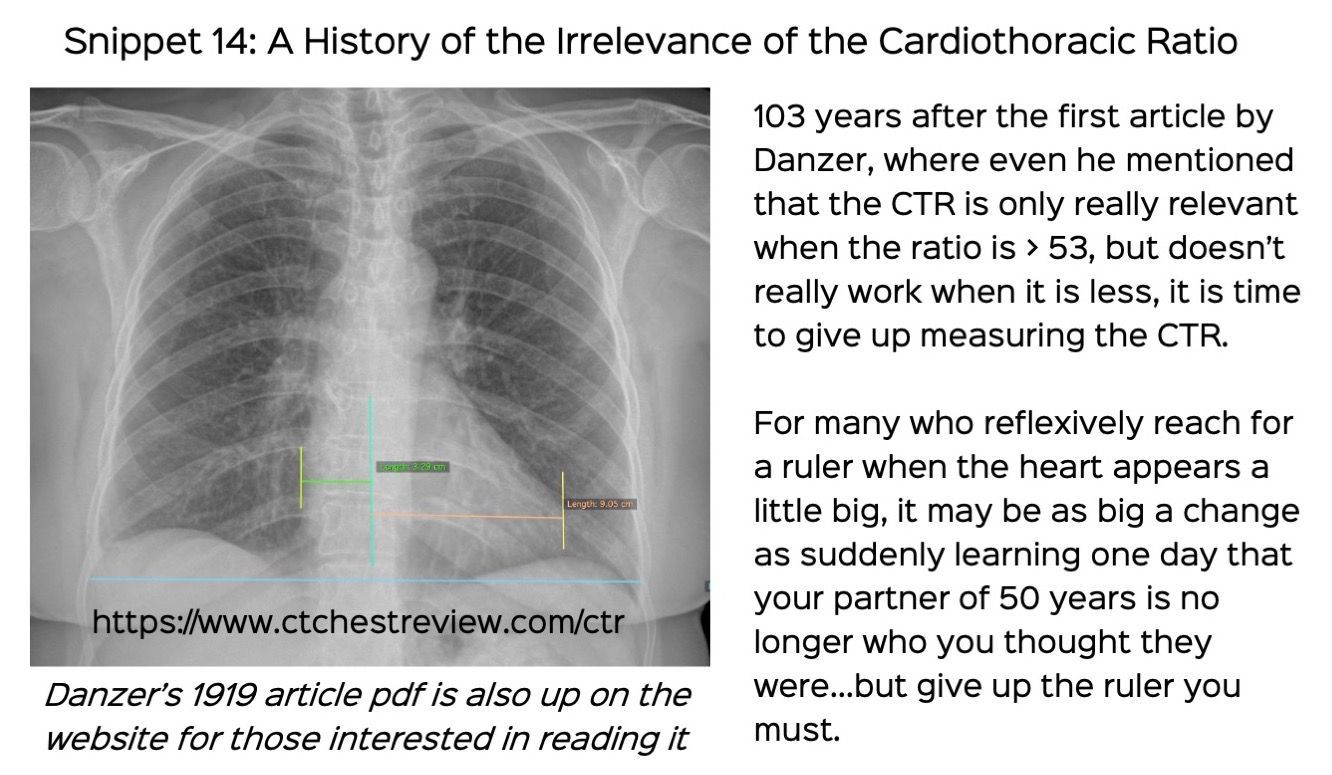
Snippet 14: A History of the Irrelevance of the Cardiothoracic Ratio
It is time to give up the cardiothoracic ratio
The first article on the cardiothoracic ratio was published in 1919 by Dr. Danzer in the American Journal of Medical Sciences. You can download it from here.
103 years ago, this is what he said and did.
- 500 patients
- Mid-inspiratory images
- Avg CTR of 45% with 2% margin of error on either side
- 53% and above considered abnormal for LV hypertrophy and dilatation
- If the ratio is not increased, LVH cannot be ruled out and other methods are needed for cardiac assessment (murmurs and history)
- Under 45% - think of tuberculosis (phthisis)
103 years later, many radiologists still reach for a ruler (physically or on screen) to measure the CTR. As far back as in 1973, Dr. Davies mentioned in JAMA that it was pretty much useless.
Two new articles in the last 6 months have further hammered the last few nails in CTR's coffin.
https://twitter.com/KateHanneman/status/1457716133935599620
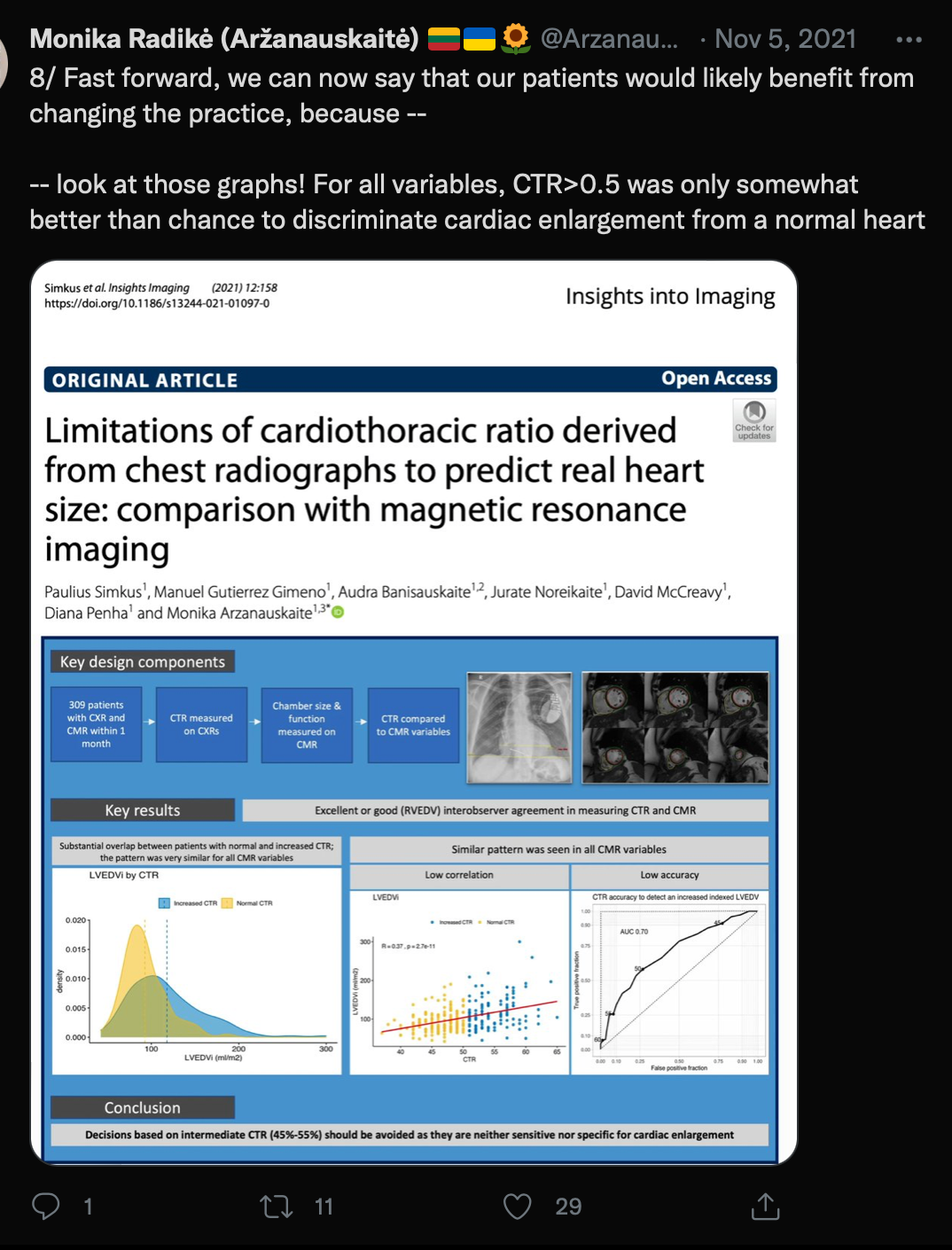
https://twitter.com/Arzanauskaite/status/1456365269195034637
Dr. Saurabh Jha from UPenn goes a step further

https://twitter.com/RogueRad/status/1048016753522036736
This blog post also philosphically addresses the issue.
 Paul McCoubrie
Paul McCoubrie
This is similar to the issue we have with measuring our body temperature, which I wrote about a few weeks ago.
 Bhavin Jankharia
Bhavin Jankharia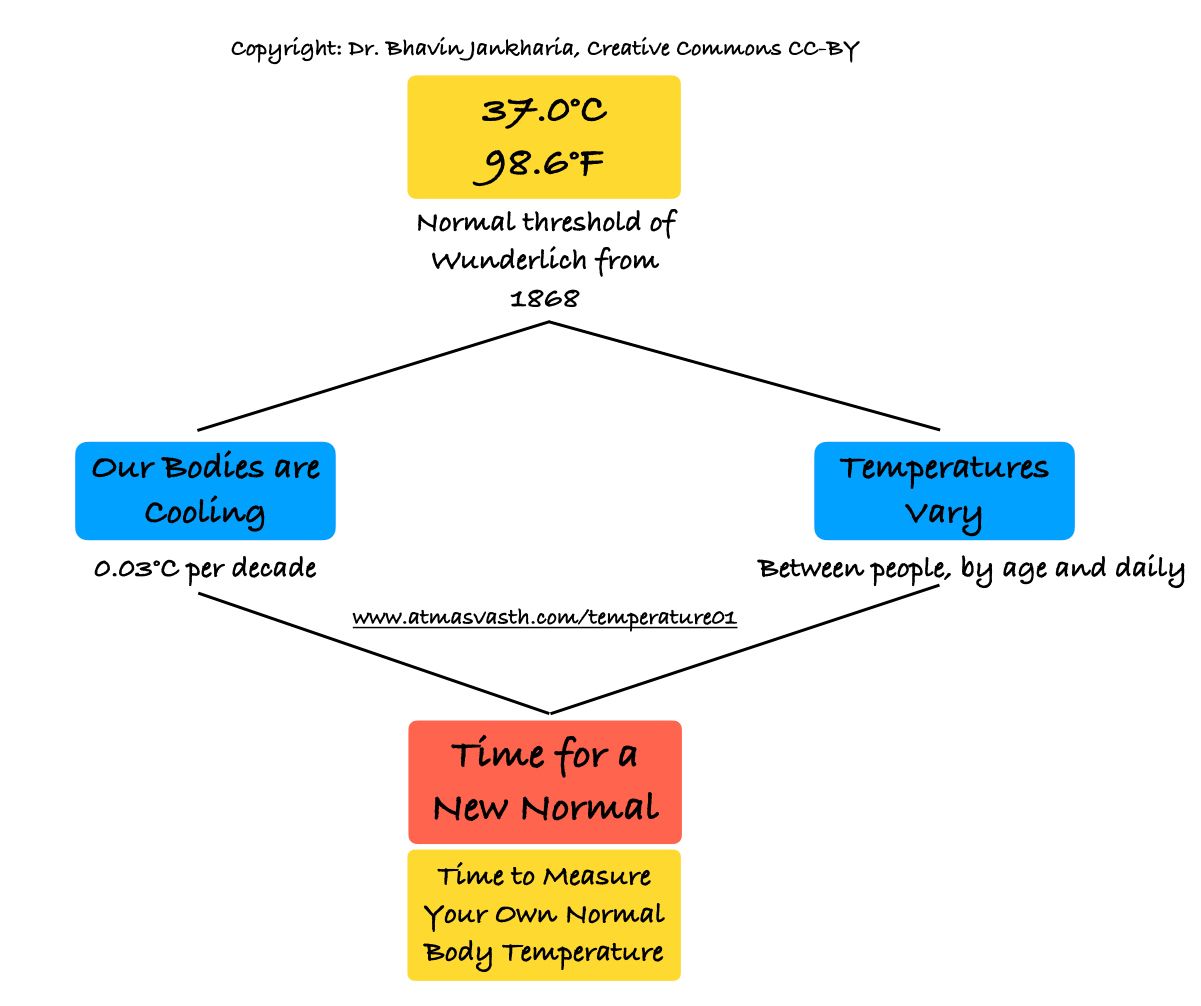
Other Posts and Sites
 Bhavin Jankharia
Bhavin Jankharia
 Bhavin Jankharia
Bhavin Jankharia
CT Chest Review Newsletter
Join the newsletter to receive the latest updates in your inbox.
{kind=link}